![]()
Articles
![]()
Otitis : what you need to know
Until the age of 4-5 years, middle ear problems in children are very common. Some doctors speak of infection, others of otitis and sometimes of liquid behind the eardrum: in any case, this pathology raises many questions for the parent!
The main reason for the abundance of otitis before children are of school age is very simple: the channel that ventilates the ear, the Eustachian tube, is immature. Its physiology is not the same as that of an adult. Horizontal and narrower, its ventilation is inefficient and insufficient. In addition, structures in the nose and throat, such as the tonsils and adenoids, may play a role. These problems can still occur in older children or adults, but they are less frequently encountered.
Types of otitis
Serous otitis
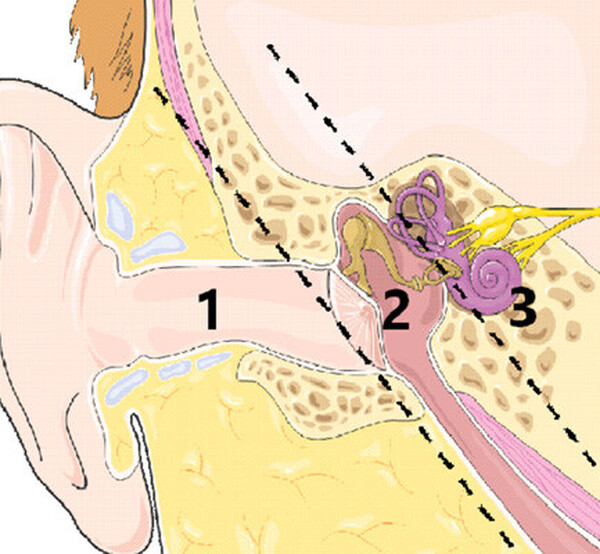
In the presence of serous otitis, uninfected fluid is found behind the eardrum, or in the middle ear (2). The child does not have a fever, and since it is not an infection, no antibiotics are needed. Serous otitis is often called "silent otitis" because it causes few or no noticeable symptoms. At a young age, the child is not able to verbalize it: the slightly older child may complain of a feeling of clogged ears, due to the presence of liquid.
Acute otitis media
In the presence of acute otitis media (AOM), infected fluid is found in the middle ear (2). The latter was infected by microbes from the throat and nose, which arrived there through the Eustachian tube. As it is an infection, an antibiotic medicine can be prescribed to the child by his attending physician.
otitis externa
Otitis externa or "swimmer's ear" is an infection of the external auditory canal (1). In these specific cases, there is no liquid found behind the eardrum. However, otitis externa can still cause temporary hearing loss.
Impacts on hearing
The focus of the audiologist is hearing loss associated with the presence of fluid (infected or not) in the middle ear. This can be light or moderate, depending on the amount of liquid.
If fluid remains, the temporary deafness may last for several months, fluctuating depending on the condition of the middle ear. A child with a chronic ear infection problem may experience a language delay or learning difficulties: restricted access to vocabulary, due to hearing loss, affects cognitive development.
Take the test: wear noise protection earplugs and try to understand your interlocutors… Difficult? This is what many children experience!
Possible interventions
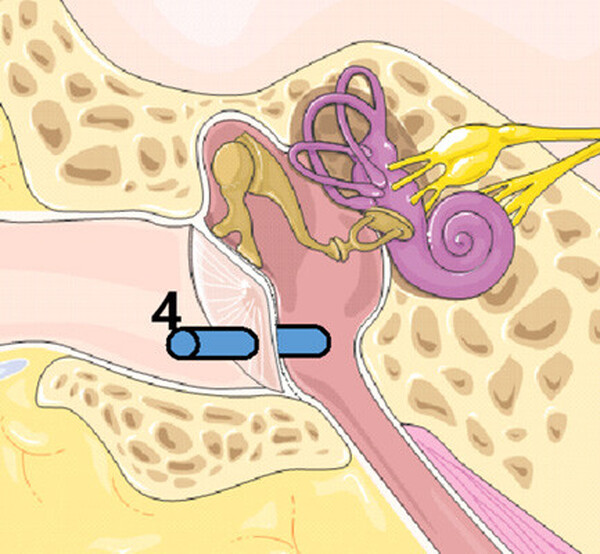
When the problem is recurrent, the doctor identifies chronic otitis media. Diagnostic criteria often vary from doctor to doctor. If no antibiotic and/or nasal hygiene protocol works, then the practitioner suggests a myringotomy with insertion of tubes (4).
This minor surgery involves making a small incision in the eardrum and placing a small tube, also called a coil or drain, through it. The goal is to ensure ventilation of the ear through the external route.
The procedure is usually done under general anesthesia: young children move too much for it to be done in an outpatient clinic under local anesthesia.